- Resource
- BR1DGE
- Early Detection
- Article
ATTD 2026 Symposium Summary
In this panel Prof. Alice Cheng facilitated a comprehensive discussion with Drs. Sanjoy Dutta, Jeremy Pettus, Jessica Melin, Karin Lange and Renuka Dias. Through role-played scenarios, the speakers explored the T1D care journey from screening and diagnosis to monitoring and management, highlighting the real-world disease burden and the critical importance of early detection. The panel also reviewed current technologies and key decision points that enable effective T1D care.
This article is intended to be a summary only. Additional topics were covered in the live symposium in line with the applicable regulations but are not included on the BR1DGE platform.

Meeting Objectives
- Highlight the real-world burden of T1D, emphasizing the clinical importance of screening, early detection, and multidisciplinary management
- Illustrate via expert-led case studies the full breadth of the T1D care journey from screening and diagnosis through to monitoring and management
- Reflect on key decision points in the T1D care journey, identify next steps, and discuss available management options
Symposium Faculty






Early Detection and Screening

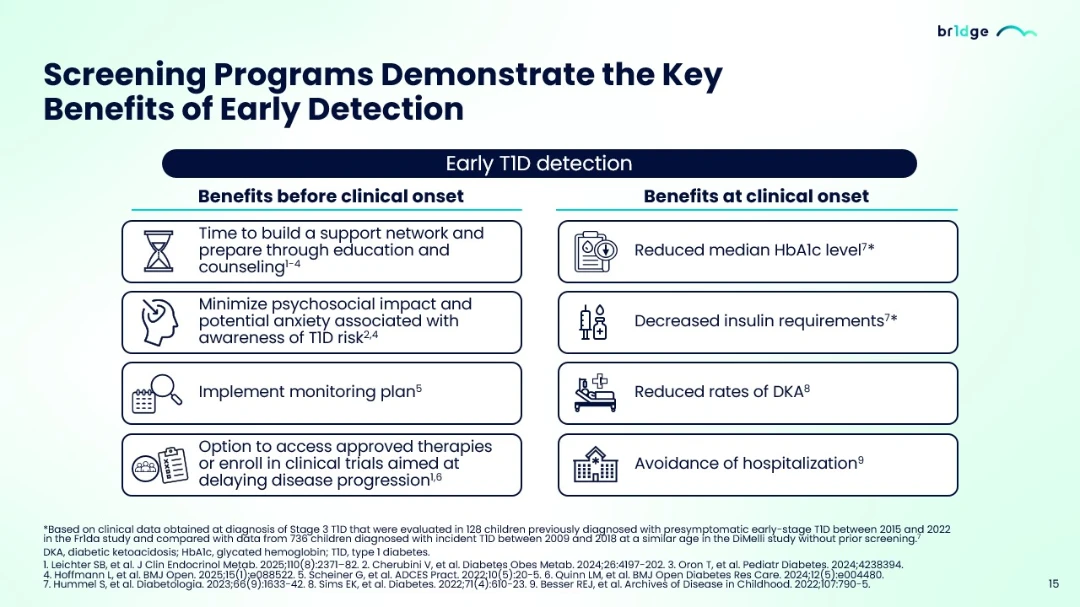
“If you go through screening and monitoring, it has been observed that DKA percentage rates are significantly reduced to single digit percentage. Also, there is a lower HbA1c level and better management of HbA1c with reduced insulin need here and you can also avoid the hospitalization.”
- The global burden of T1D is rising, with nearly half of new diagnoses occurring in adults. Approximately 40% of adults who develop T1D after 30 years of age are initially misclassified as having T2D, thus delaying appropriate treatment, despite first-degree relatives having up to a 15-fold higher risk of developing T1D1,2
- The risk of cardiovascular complications increases with earlier progression to Stage 3, and the prevalence of DKA at T1D onset remains alarmingly high3,4
- Individuals with co-existing autoimmune conditions such as celiac disease or autoimmune thyroiditis face a 2.5–3-fold elevated risk of developing T1D compared to the general popoulation5
- Early screening using islet autoantibodies offers significant clinical value: lower rates of DKA at diagnosis,6 improved glycemic control with reduced HbA1c levels,7 and earlier opportunities to participate in clinical trials or approved therapies8,9
- Early T1D detection minimizes the psychological impact and potential anxiety associated with the diagnosis of T1D while providing time to build support networks and prepare through education and counselling9-11
- Major T1D organizations (ADA, FR1DA, GPPAD, ISPAD) provide guidance for both clinicians and individuals who are undergoing screening. The BR1DGE program supports guidance on screening as well as other resources to help HCPs provide effective T1D care12-17
- Ongoing efforts at Breakthrough T1D include developing enhanced genetic risk scores and building the evidence base for cost-effective, population-wide screening, with the long-term goal of driving policy-level change globally18
Bridging the Gap: Interpreting & Communicating Autoantibody Results

“The general rule of thumb is that you should probably screen these people again maybe in six months, a year to see what happens because some of these people revert to autoantibody negative, some will go on to have more autoantibodies.”
- IAA, IA-2A, GADA, ZnT8A are the four primary islet autoantibodies used in T1D screening. The availability of IAbs means individuals can be screened to detect and diagnose early-stage T1D1-4
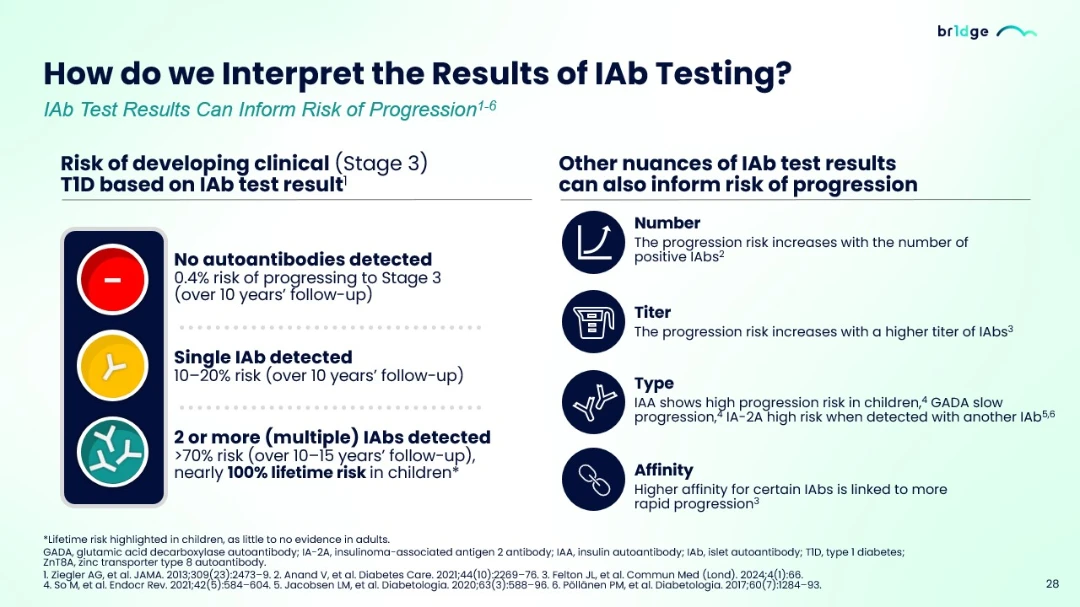
- IAbs testing helps predict T1D progression risk: no autoantibodies indicate 0.4% risk, single autoantibodies show 10–20% risk, and 2 or more autoantibodies indicate >70% risk with nearly 100% lifetime risk in children5-10
- Beyond the number of positive autoantibodies, several factors influence progression risk: IAA demonstrates high progression risk in children, GADA typically indicates slower progression, and IA-2A signals elevated risk when detected alongside other autoantibodies13
- International guidelines and international diabetes societies (ISPAD, Breakthrough T1D, ADA, EDENT1FI) emphasize the importance of confirmatory testing protocols. Positive results should be verified in a second sample, preferably through an independent reference laboratory, to confirm persistence of the autoimmune response and improve diagnostic accuracy3,11-13
- IAb testing facilitates critical differentiation between T1D and T2D in adults. Current ADA guidelines recommend autoantibodies testing in suspected adult-onset T1D cases, integrated with C-peptide measurement and clinical assessment. The AABBCC clinical approach provides a structured framework for distinguishing T1D based on key clinical characteristics13
Sustaining the Continuum: Monitoring, Education & Preparing for Progression

“The most important one is that we will try to prevent DKA among those patients. We want them to have a smooth landing with less symptoms and less serious complications. But monitoring also gives us a very good opportunity to educate and inform these families, these teenagers and young adults, regarding type 1 diabetes”

“'m as you working primarily with families with children with Stage 1 and 2, the anxiety is more in the mothers, less in the fathers and the even the younger children don't understand what's happening to them, but they have a feeling that something is different.”
- It is important to maintain ongoing monitoring for individuals in Stage 1 and Stage 2 T1D, noting that monitoring may extend over several years1
- The principal aims of monitoring and management in early-stage T1D include preventing DKA and minimizing the requirement of emergency care, providing comprehensive support and education to reduce anxiety while increasing symptom awareness, and offering guidance for insulin therapy initiation to mitigate long-term complications1
- Early-stage T1D monitoring provides substantial clinical advantages. Lower DKA rates at diagnosis correlate with superior long-term glycemic control. Additional benefits include reduced hospitalization rates, mitigation of DKA related complications, decreased hyper- and hypoglycemia episodes, and milder diabetes presentation at clinical onset in pediatric populations2-9
- Importantly, monitoring creates opportunities for patient education and counseling while allowing time to develop essential glycemic management skills before insulin dependence10-12
- Early detection and monitoring present a dual impact on psychosocial burden. During Stages 1 and 2, individuals may experience progression-related anxiety and confusion, including parental anxiety regarding monitoring responsibilities, fear of the unknown concerning disease severity and insulin requirements, and reduced engagement due to concerns about lifelong management impacts on education, career, relationships, and insurability10-12
- Conversely, screening enables psychological preparation for Stage 3 progression. Gradual psychological adjustment may reduce the shock associated with clinical onset. Additionally, screening reduces DKA risk at diagnosis, representing a significant clinical and psychological benefit10-12
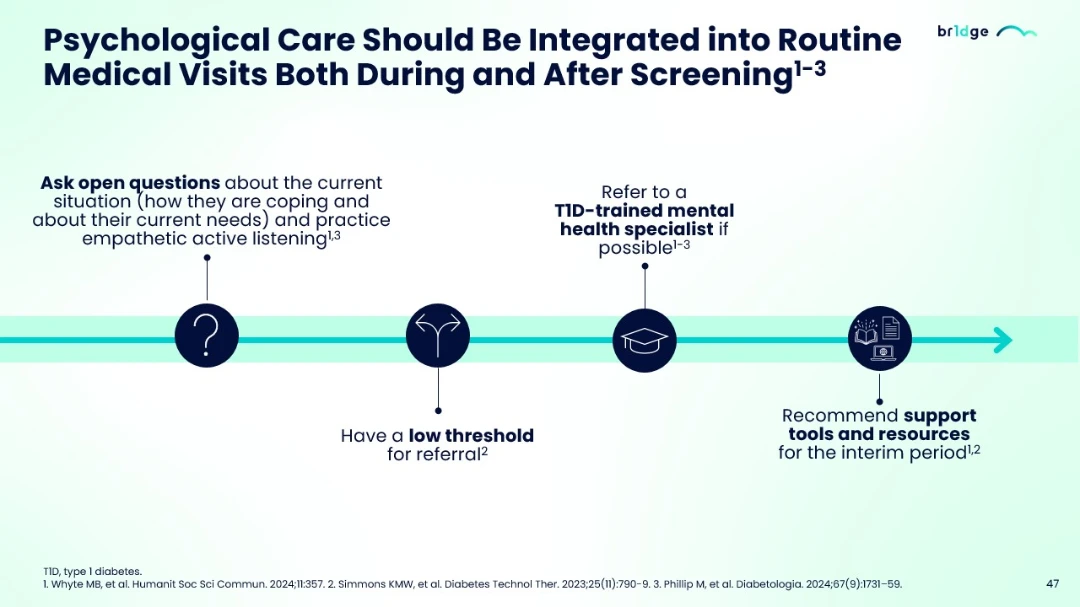
- Psychological care must be integrated into routine medical visits throughout the screening and monitoring continuum. Healthcare professionals should employ open-ended questioning about coping mechanisms and current needs while practicing empathetic active listening1,13,14
- Maintaining a low threshold for referral to T1D-trained mental health specialists is essential, with interim support tools and resources recommended when specialist access is limited14
Evolving Approaches to T1D Management & Treatment Options

“We have this unique opportunity to become proactive in our management, and this is where disease-modifying therapies which have the potential to preserve beta cell function and in early-stage and new-onset type 1 diabetes can come into play.”
- Despite advances in glucose monitoring and insulin delivery technologies, individuals with T1D continue to face substantial disease burden, with only approximately 36% achieving time-in-range goals. This emphasizes the need for a proactive approach targeting early-stage disease to address persistent inequities in outcomes1,2-5
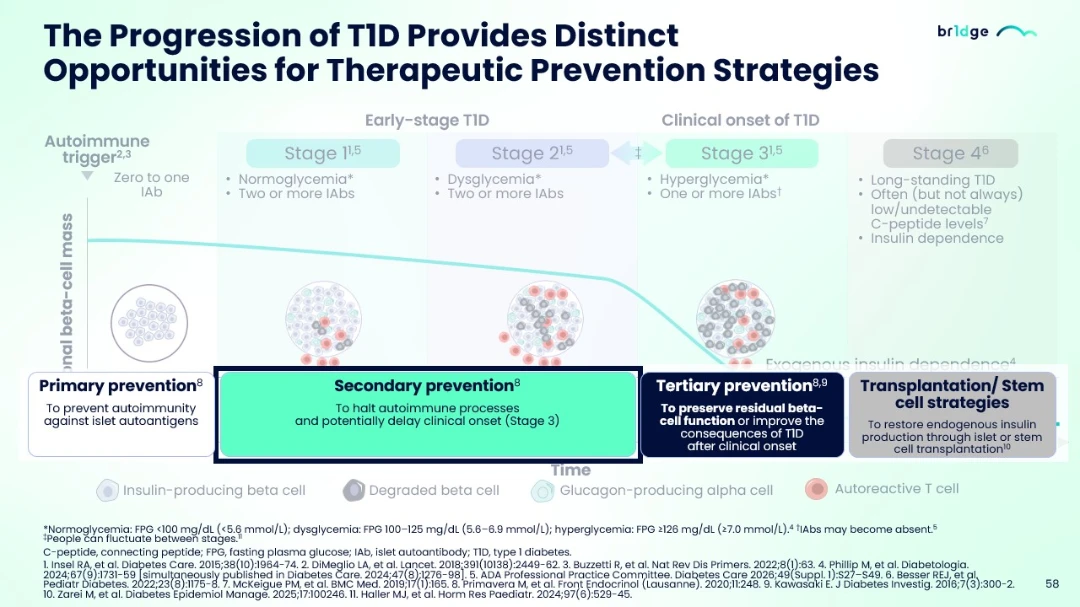
- The contemporary understanding of T1D progression through distinct stages provides multiple intervention opportunities3,6-11
- Four distinct prevention approaches are under investigation: primary prevention aims to prevent autoimmunity against islet autoantigens; secondary prevention seeks to halt autoimmune processes and delay Stage 3 onset; tertiary prevention focuses on preserving residual beta-cell function post-clinical onset; and transplantation/stem cell strategies aim to restore endogenous insulin production6-11
- Multiple immunomodulatory investigational strategies are targeting various immune pathways including T-cell modulation, regulatory T-cell enhancement, and antigen-specific tolerance induction16-31
- The broad pipeline of immunotherapies targeting T-regulatory cells, T-effector cells, cytokines, and B cells is under investigation16-31
- Advances in staging, screening, and early detection have fundamentally transformed T1D management, enabling proactive intervention strategies before clinical symptom onset and offering potential disease modification opportunities16-31
Author Disclosure: At the time of this presentation, Alice Cheng declared research funding from Applied Therapeutics, Novo Nordisk and Sanofi; Speaker/Consultant from Abbott, Amgen, Astellas, Aspen, Bausch, Bayer, Biomea, Boehringer Ingelheim, Caliway Biopharmaceuticals, Dexcom, Eisai, Eli Lilly, Gan & Lee, GSK, Insulet, HLS Therapeutics, Medtronic, Merck, MSD, Novo Nordisk, Pfizer, Sandoz, Sanofi, Vertex. Sanjoy Dutta had no research funding and was a speaker or consultant for Breakthrough T1D, New York, USA. Jeremy Pettus was a speaker or consultant for Novo Nordisk, Sanofi, Eli Lilly, Carmot Therapeutics, Diasome, Kriya, and Biomea Fusion. Jessica Melin was a speaker or consultant for Sanofi and Karin Lange was a speaker or consultant for Abbott, AstraZeneca, BDI, BioMarin, Chiesi, Glooko, Insulet, Lilly, Medtronic, Merck Serono, MSD SHARP & DOHME, Novo Nordisk, Roche Diabetes Care, Sanofi.
MAT-GLB-2602539 – 1.0 – 05/2026
Early Detection and Screening
1. Holt RIG, et al. Diabetes Care. 2021;44:2589–625.
2. Munoz C, et al. Clin Diabetes. 2019;37(3):276–81.
3. Chiesa ST, et al. Front Pediatr. 2021:696499.
4. Alonso GT, et al. Diabetes Care. 2020;43:117–21.
5. Edelman SV, et al. Diabetes Obes Metab. 2025;27(8):4229–38.
6. Sims EK, et al. Diabetes. 2022;71(4):610–23
7. Hummel S, et al. Diabetologia. 2023;66(9):1633–42
8. Besser REJ, et al. Archives of Disease in Childhood. 2022;107:790–5
9. Leichter SB, et al. J Clin Endocrinol Metab. 2025;110(8):2371–82.
10. Cherubini V, et al. Diabetes Obes Metab. 2024;26:4197-202.
11. Oron T, et al. Pediatr Diabetes. 2024;4238394.
12. Hoffmann L, et al. BMJ Open. 2025;15(1):e088522.
13. Phillip M, et al. Diabetologia. 2024;67(9):1731–59.
14. ADA. Diabetes Care. 2026;49(Suppl 1):S50-S60.
15. Hendriks AEJ, et al. Diabetes Metab Res Rev. 2024;40(2):e3777.
16. Haller MJ, et al. Horm Res Paediatr. 2024;97(6):529–45.
17. Martínez-Brocca MA, et al. Endocrinol Diabetes Nutr (Engl Ed). 2025;72(9):501639.
18. Breakthrough T1D. Advancing Genetic Risk Assessment for Type 1 Diabetes: Improving Prediction and Clinical Translation. Available at: https://www.breakthrought1d.org/wp-content/uploads/2025/05/RFA_GRS_Call-Document_final-v.pdf. Accessed Mar 2026.
Bridging the Gap: Interpreting & Communicating Autoantibody Results
1. Winter WE, et al. J Appl Lab Med. 2022;7:197–205.
2. Bonifacio E, Achenbach P. Clin Exp Immunol. 2019;198(3):294–305.
3. Phillip M, et al. Diabetologia. 2024;67(9):1731-59.
4. Peters A. J Fam Pract. 2021;20;Suppl:S47-S52.
5. Ziegler AG, et al. JAMA. 2013;309(23):2473–9.
6. Anand V, et al. Diabetes Care. 2021;44(10):2269–76.
7. Felton JL, et al. Commun Med (Lond). 2024;4(1):66.
8. So M, et al. Endocr Rev. 2021;42(5):584–604.
9. Jacobsen LM, et al. Diabetologia. 2020;63(3):588–96.
10. Pöllänen PM, et al. Diabetologia. 2017;60(7):1284–93.
11. Haller MJ, et al. Horm Res Paediatr. 2024;97(6):529–45.
12. Hoffmann L, et al. BMJ Open. 2025;15(1):e088522.
13. ADA. Diabetes Care. 2026;49(Supp1):S27–S49.
Sustaining the Continuum: Monitoring, Education & Preparing for Progression
1. Phillip M, et al. Diabetologia. 2024;67(9):1731-59.
2. Hendriks AEJ, et al. Diabetes Metab Res Rev. 2024;40(2):e3777.
3. Besser REJ, et al. Arch Dis Child. 2022;107:790-5.
4. Scheiner G, et al. ADCES in Practice. 2022;10(5):20-5.
5. Barker JM, et al. Diabetes Care. 2004;27(6):1399-404.
6. Duca, LM, et al. Diabetes Care. 2017;40:1249-55.
7. Karges B, et al. Diabetes Care. 2021;44(5):1116-24.
8. Niechial E, et al. Sci Rep. 2026. doi: 10.1038/s41598-026-38533-4. Online ahead of print.
9. Hummel S, et al. Diabetologia. 2023;66:1633-42.
10. Bennet Johnson S, et al. Curr Diab Rep. 2011; 11:454-9.
11. O’Donnell H. et al. Diabetes Care 2023;46(12):2155–2161
12. Leichter SB, et al. J Clin Endocrinol Metab. 2025;110(8):2371-82.
13. Whyte MB, et al. Humanit Soc Sci Commun. 2024;11:357.
14. Simmons KMW, et al. Diabetes Technol Ther. 2023;25(11):790-9.
Evolving Approaches to T1D Management & Treatment Options
1. Dovc K, et al. JAMA Network Open. 2023;6(2):e23007.
2. Powers AC. J Clin Invest. 2021;131(8):e142242.
3. Insel RA, et al. Diabetes Care. 2015;38(10):1964-74.
4. Besser REJ, et al. Arch Dis Child. 2022;107:790–5
5. Herold KC, et al. Nat Rev Immunol. 2024;24(6):435-51.
6. DiMeglio LA, et al. Lancet. 2018;391(10138):2449-62.
7. Buzzetti R, et al. Nat Rev Dis Primers. 2022;8(1):63.
8. Phillip M, et al. Diabetologia. 2024;67(9):1731-59.
9. ADA Diabetes Care 2026;49(Suppl. 1):S27–S49.
10. Besser REJ, et al. Pediatr Diabetes. 2022;23(8):1175-8.
11. McKeigue PM, et al. BMC Med. 2019;17(1):165.
12. Primavera M, et al. Front Endocrinol (Lausanne). 2020;11:248.
13. Kawasaki E. J Diabetes Investig. 2016;7(3):300-2.
14. Zarei M, et al. Diabetes Epidemiol Manage. 2025;17:100246.
15. Haller MJ, et al. Horm Res Paediatr. 2024;97(6):529-45.
16. Jacobsen LM, et al. Curr Diab Rep. 2018;18(10):90.
17. Houeiss P, et al. Front Endocrinol (Lausanne). 2022;13:933965.
18. Boldison J, Wong FS. Front Immunol. 2021;12:746187.
19. Su B, et al. Front Immunol. 2025:16:1571247.
20. Russell WE, et al. Diabetes Care. 2023;46(5):1005–13.
21. ClinicalTrials.gov. NCT05757713. Accessed Feb 2026.
22. Herold KC, et al. N Engl J Med. 2019;381(7):603-13.
23. Libman I, et al. Diabetes Care. 2023;46(11):2035-43.
24. ClinicalTrials.gov. NCT06688331. Accessed Feb 2026.
25. ClinicalTrials.gov. NCT01122446. Accessed Feb 2026.
26. ClinicalTrials.gov. NCT02611232. Accessed Feb 2026.
27. Penaforte-Saboia JG, et al. Diabetes Metab Syndr Obes. 2024;17:857-6.
28. ClinicalTrials.gov. NCT05219409. Accessed Feb 2026.
29. Gale EAM, et al. Lancet. 2004;363(9413):925-31.
30. ClinicalTrials.gov. NCT07222137. Accessed Feb 2026.
31. Teizeild (Teplizumab) SmPC. January 2026.